You may be here because your mother says she's fine, but you've noticed the unopened mail, the near fall in the bathroom, or the way she gets winded walking from the kitchen to the car. Nothing looks dramatic on its own. Together, they can signal risk.
That's what the term high risk population should mean to a family caregiver. Not a label. Not a reason to panic. A way to notice who is more likely to struggle, decline, or hit a crisis unless someone steps in early.
In practice, caregivers rarely deal with one clean problem. They deal with stacks of small ones. A heart condition plus missed refills. Arthritis plus stairs. Memory changes plus living alone. The work is learning which combinations matter most, and what to do before the next urgent call forces the issue.
What Does High Risk Population Mean for Your Family
A family usually starts using this language after something small feels bigger than it should.
Your father misses one specialist visit because he couldn't drive that day. Your aunt stops cooking because standing hurts. Your spouse shrugs off dizziness because they “just got up too fast.” None of that sounds like a crisis. But if those problems sit there long enough, they become one.
For caregivers, a high risk population isn't just “older people” or “people with a diagnosis.” It's a group of people more likely to have poor outcomes because of a mix of health conditions, care gaps, and daily-life barriers. The useful part of the term is that it gets you to stop asking only, “What disease do they have?” and start asking, “What could cause them to get worse?”
A point many families miss is the difference between high risk and underserved. A person can be medically high risk because of a condition or a cluster of conditions, but still have excellent insurance, nearby specialists, and reliable transportation. Someone else may not look medically fragile at first glance, yet still be underserved because getting appointments, medications, or basic follow-up is hard due to access and quality barriers tied to social factors. That distinction is outlined in a Johns Hopkins and MD Anderson review on underserved versus high-risk populations.
What this looks like in real life
Here are three common versions of “high risk” I see families miss:
- The capable parent with hidden complexity. They still drive and hold a conversation well, but they manage several medications badly and skip meals.
- The younger adult with chronic illness. They're still working, so relatives assume they're stable, but their condition is one missed follow-up away from a setback.
- The isolated older neighbor. The diagnosis list may be short, but poor support turns ordinary problems into emergencies.
Practical rule: If you're noticing patterns instead of single incidents, stop thinking in terms of “fine” versus “not fine.” Start thinking in terms of risk.
That shift helps you act earlier, and with a lot less chaos.
Understanding Medical Social and Environmental Risks
Most caregivers focus first on medical problems because those are easiest to name. Diagnosis. Medications. Appointments. But risk rarely stays in one lane.
A better way to assess a high risk population is to think in three buckets: medical, social, and environmental. If you want a simple analogy, medical risk is the engine, social risk is the support system, and environmental risk is the road the person has to travel every day.
Medical risk
Medical risk includes the issues most families expect:
- Chronic conditions such as heart disease, diabetes, COPD, or cancer
- Multiple medications that can be confused, duplicated, or skipped
- Mobility limits that make bathing, dressing, or getting to appointments harder
- Symptoms that fluctuate like dizziness, fatigue, shortness of breath, or confusion
The trap is assuming diagnosis alone tells you how worried to be. It doesn't. Two people can both have diabetes, but one is stable and organized while the other has vision loss, missed refills, and no reliable meals. Their risk isn't the same.
If you're sorting out whether your relative is more broadly vulnerable, it can help to read a plain-language guide on what medically frail means. Frailty overlaps with risk, but it isn't the whole picture.
Social risk
Social risk is where many care plans fail.
Columbia Nursing notes that high-risk groups often face chronic conditions, worse access to care, and higher morbidity, which is why screening for barriers like transportation matters as much as the diagnosis itself in many cases, as described in its overview of high-risk, underserved, and vulnerable populations.
Social risk can include:
- Living alone with no one noticing decline
- Transportation problems that turn routine care into missed care
- Financial strain that leads to rationing medication or delaying treatment
- Caregiver burnout when one family member does everything
- Low trust in the system after bad past experiences
Environmental risk
This is the bucket families underestimate most because the home looks normal to them.
A steep front step, dim hallway, loose rug, heavy laundry basket, cluttered path to the bathroom, and no grab bar in the shower can turn a manageable condition into a fall, a hospitalization, or a permanent loss of confidence.
A person doesn't need to be very sick to be unsafe. They just need one bad setup on one bad day.
When medical, social, and environmental risks pile together, trouble speeds up. That's why the strongest caregiver decisions usually come from looking at the whole living situation, not just the chart.
Your Caregiver Checklist for Identifying Key Risks
A checklist beats a vague worry every time. It gives you something you can observe, write down, and bring to a doctor, sibling, home care agency, or social worker.
A useful reason to do this thoroughly is that risk reaches far beyond the people families instinctively label as “frail.” A 2021 NHANES-based analysis estimated that 176.1 million U.S. adults, or 75.4%, had at least one condition associated with increased risk of severe COVID-19 illness, and 69.2% of adults under 65 were also considered at increased risk in that framework, according to the published analysis of U.S. adult risk prevalence. For caregivers, the lesson is simple. Don't assume younger or outwardly independent means low risk.
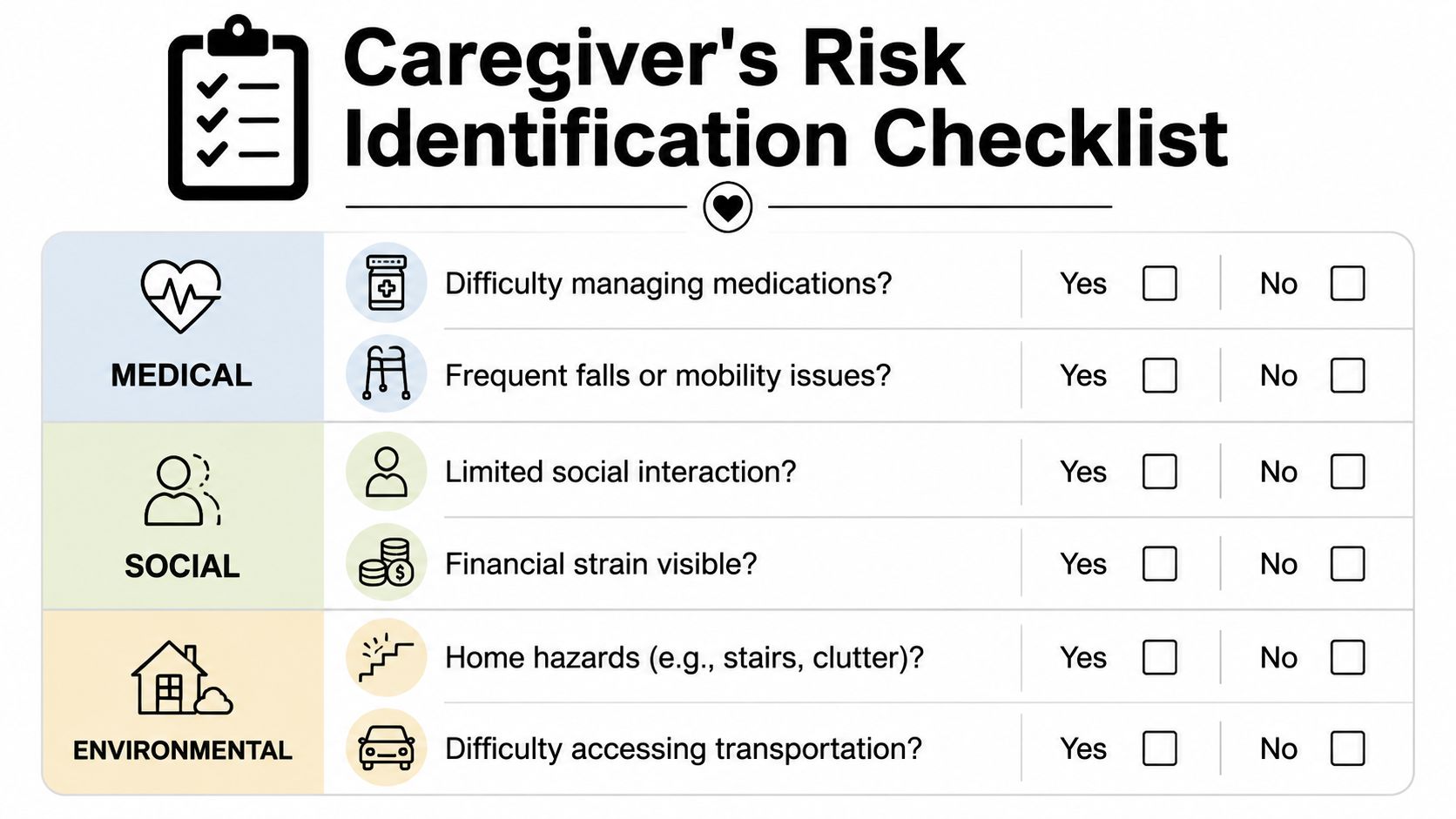
Medical warning signs to document
Ask yourself:
- Medication confusion: Does your loved one miss doses, double doses, run out early, or keep old pill bottles “just in case”?
- Recent changes: Have you noticed new weakness, shortness of breath, swelling, dizziness, appetite loss, or memory lapses?
- Mobility trouble: Are they holding furniture to walk, avoiding stairs, or moving differently than they did a month ago?
- Care gaps: Are they overdue for follow-up, avoiding specialists, or canceling appointments because getting there is too hard?
- Recovery problems: After an illness or hospital stay, did they bounce back, or never really return to baseline?
If several of those are true, write examples with dates. “Forgot evening pills twice this week” is more useful than “bad with meds.”
For a home-focused way to think through layered danger, I also like using a simple hazard vulnerability analysis mindset. It helps families rank what could go wrong, what's most likely, and what would hurt the most.
Here's a short video that can help you think through practical safety concerns in a caregiving setting:
Social and daily-life risks to notice
These are often the difference between stable and spiraling:
- Isolation: Who sees or speaks with them regularly, and who would notice a bad day?
- Food access: Is there actual food in the home that they can prepare and will eat?
- Money strain: Are bills stacking up, utilities at risk, or copays becoming a reason to skip care?
- Decision overload: Do forms, portals, and phone calls confuse them enough that tasks don't get done?
- Backup support: If you got sick tomorrow, who would step in?
Environmental issues to walk through in person
Don't assess this from the couch. Walk the home.
| Area | What to check | Why it matters |
|---|---|---|
| Bathroom | Tub entry, slippery floors, no grab bars, low toilet | Falls happen fast in tight spaces |
| Bedroom | Distance to bathroom, clutter, poor lighting, unstable furniture | Nighttime confusion and rushing increase risk |
| Kitchen | Spoiled food, hard-to-reach dishes, heavy cookware | Daily tasks become injury points |
| Entryways | Steps, railings, uneven surfaces, packages on floor | One missed footing can change everything |
If your checklist is getting long, that doesn't mean you failed. It means you can finally see the workload clearly.
A good checklist doesn't solve the problem. It gives you a starting map.
Prioritizing Concerns and Building a Care Plan
Once you've listed the risks, don't try to fix everything in one weekend. That's how caregivers burn out and relatives shut down.
Health systems use data to stratify risk and decide where to intervene first. Families can do a simpler version of the same thing by gathering information across medical, social, and environmental factors, then focusing first on the issues most likely to cause harm, as described in this overview of risk stratification and interventions for high-risk patient populations.

Triage first
Use a simple three-part filter:
- What could cause immediate harm
Falls, medication errors, wandering, unsafe driving, chest symptoms, inability to get help - What is causing steady decline
Missed meals, skipped appointments, unmanaged pain, worsening mobility, caregiver exhaustion - What is stressful but can wait briefly
Closet cleanup, paperwork organization, non-urgent home updates
Families often get stuck. They spend two hours arguing about whether to repaint the bedroom while no one has fixed the shower setup or sorted the pill bottles.
Build a one-page plan
Keep it short enough that people will use it. A good first care plan can fit on one page.
Include:
- Top three risks
Example: bathroom falls, medication confusion, missed cardiology follow-up - Immediate actions
Example: remove rugs, set up a weekly pill organizer, call office for next appointment - Who owns each task
One sibling handles scheduling, one handles the home visit, one handles pharmacy pickup - What to monitor
Appetite, walking changes, swelling, missed doses, mood, sleep - When to review
Pick a date and stick to it
What works and what usually doesn't
Works well
- Written plans shared with siblings
- One person designated as the main coordinator
- Tasks assigned by role, not by vague goodwill
- A short follow-up call after each appointment
Usually fails
- “We'll all help however we can”
- Long email threads with no owner
- Buying equipment before checking whether the person will use it
- Trying to solve resistance and logistics on the same day
If you want a practical tool for this stage, Family Caregiving Kit offers worksheets for home safety and emergency preparedness that can help you turn observations into a usable action list rather than loose notes.
Simple Strategies to Prevent and Reduce Risks
Most good risk reduction is not dramatic. It's repetitive, boring, and effective.
That's good news for caregivers because the highest-value changes are often simple. You don't need a perfect system. You need one your loved one can live with.
Medical risks you can reduce at home
- Medication reminders: Use a weekly pill organizer, pharmacy blister packs, or phone alarms. If the person ignores alarms, tie medication to an existing habit like breakfast or brushing teeth.
- Single medication list: Keep one updated list on paper and on a phone. Bring the same list to every appointment.
- Symptom tracking: Use a notebook for appetite, pain, dizziness, bowel changes, and sleep. Doctors can work with patterns. They can't do much with “she's just off.”
- Simplify follow-up: Book the next appointment before leaving the current one whenever possible.
Social risks that quietly drive decline
- Regular check-ins: A short predictable call often works better than random long calls. Routine beats intensity.
- Food support: Stock easy meals that don't require heavy pans or complicated prep.
- Shared family calendar: Keep visits, refills, rides, and lab work in one place so tasks don't vanish.
- Respite planning: If one caregiver is carrying too much, arrange backup before resentment and exhaustion take over.
What helps most: Small supports that happen every week usually matter more than heroic efforts once a month.
Environmental changes with high payoff
Start with the places where people rush or lose balance.
- Bathroom: Add a non-slip mat, improve lighting, and install grab bars where transfer support is needed. If you need examples of safe placement and common setup mistakes, this Vancouver grab bar installation guide is a practical reference.
- Pathways: Remove loose rugs, trailing cords, unstable side tables, and piles of shoes or laundry.
- Night safety: Put a lamp within reach of the bed or use motion-sensor lighting on the route to the bathroom.
- Entry access: Make sure railings are sturdy and commonly used steps are clear.
When access to care is limited
In underserved settings, the question often concerns what can be done with the options you have. Literature on medically underserved populations points to telehealth, mobile services, and community outreach as practical ways to bridge care gaps, especially when provider shortages or distance make standard care harder to reach, as discussed by the Health Equity and Policy Lab on underserved populations and areas.
Try concrete steps like these:
- Set up one device for virtual visits and keep the charger in the same place
- Call senior centers or faith communities to ask about rides, meal support, or wellness checks
- Ask clinics about mobile services or outreach staff instead of assuming they don't exist
- Prepare questions before telehealth visits so the appointment doesn't get wasted on setup confusion
Navigating Conversations and Legal Planning
Risk management falls apart when families avoid hard conversations for too long.
The mistake is waiting for a crisis to force honesty. By then, everyone is scared, tired, and defensive. You'll get better results if you raise concerns while your loved one can still participate in decisions.
How to talk without starting a fight
Lead with observations, not judgments.
Instead of saying, “You can't live like this anymore,” try:
“I noticed the stairs are getting harder and the shower feels unsafe. I want to make this easier, not take control away from you.”
That approach works because it names a problem the person can picture. It also lowers the chance that they'll hear the conversation as a verdict on their independence.
When siblings are involved, be direct about roles. One person can be point for medical calls. Another can handle bills. Another can do the weekly in-person check. Families do better when responsibilities are visible.
Legal planning is part of safety planning
A healthcare proxy and power of attorney are not paperwork for later. They are risk tools for now.
If your loved one ends up in the hospital, has sudden confusion, or can't manage finances temporarily, you need clear authority for decisions and logistics. Without that, even supportive families can get blocked by institutions or bogged down in conflict.
A plain-language primer on what a durable power of attorney is can help you prepare for that conversation before urgency takes over.
Focus on these basics:
- Who can make healthcare decisions if needed
- Who can manage bills, insurance issues, and accounts
- Where key documents are stored
- Who else knows the plan
Don't aim for a perfect family meeting. Aim for a usable agreement and signed documents.
Curated Resources for Your Caregiving Journey
Most caregivers don't need more information. They need the right tool for the next decision.
If your main concern is safety, use a home walk-through worksheet and document what you see room by room. If the problem is confusion among siblings, a shared care plan and task list usually help more than another emotional group text. If the issue is overload, look for resources that reduce coordination work, not just explain eldercare in theory.
A practical stack of tools often looks like this:
- A home safety worksheet for bathroom, stairs, lighting, and mobility trouble spots
- An emergency preparedness worksheet with medications, contacts, and backup plans
- A medication tracker that can travel to appointments
- A family task list with named owners and deadlines
- A respite plan so one caregiver isn't carrying the entire system
Some families also benefit from outside administrative help. If your bottleneck is scheduling, reminders, follow-up calls, and everyday coordination, this guide to using a virtual assistant for personal tasks can help you think through whether delegated support would reduce stress in your household.
The shift you're aiming for is simple. Move from vague concern to documented risk. Move from documented risk to a short plan. Then review, adjust, and keep going.
If you need structured worksheets, practical caregiving guides, and decision tools you can use with your family, visit Family Caregiving Kit. It's built to help caregivers turn overwhelm into clear next steps.