Your mother has started saying, “I'm just getting old,” when she feels tired by lunchtime. Your father seems a little more forgetful, a little less steady on his feet, and less interested in meals or going outside. Nothing looks dramatic enough for an emergency. Still, something feels off.
Caregivers often notice these changes long before anyone can name them. That matters, because vitamin B12 and D deficiency can look a lot like ordinary aging, depression, anemia, medication side effects, or the early signs of memory decline. The result is delay. Families wait. Symptoms get explained away. A treatable problem keeps moving in the background.
I've seen this many times in older adults. A daughter worries about her mother's “slowing down,” only to learn there's a deficiency contributing to fatigue and poor balance. A spouse assumes low mood and weakness are part of retirement and chronic illness, when low vitamin levels are part of the picture. These aren't rare, oddball findings in geriatric care. They're common enough that caregivers should know what to watch for and how to ask better questions.
When It Is More Than Just a Senior Moment
A son brings his father to clinic because “he's not himself.” He isn't confused all the time. He still recognizes everyone. But he's dragging his feet more, taking longer to answer questions, and complaining that his legs feel “funny.” The family thinks maybe it's stress, maybe poor sleep, maybe aging.
Then the daughter adds one detail that changes the whole conversation. “He's also been eating less, and he's been on stomach medicine for years.”
That's how these problems often show up. Not as one dramatic symptom, but as a cluster of small changes:
- More fatigue than usual
- Low mood or less interest in daily life
- New unsteadiness
- Memory slips that seem subtle but persistent
- Aches, weakness, or tingling that don't fit one obvious cause
For caregivers, the hardest part is deciding when a “maybe” deserves a doctor's visit. My rule is simple: when the change is new, persistent, or out of character, don't settle for “that's just aging” as the full answer.
Practical rule: Aging can change energy, strength, and memory. It shouldn't automatically explain a noticeable drop in function.
Vitamin B12 and vitamin D also get confusing because they can overlap. One may show up more through nerve, thinking, or mood changes. The other may show up more through muscle weakness, bone discomfort, or trouble getting around. In real life, older adults don't read textbook symptom lists. They show up with mixed complaints, multiple medications, and a family member saying, “Something isn't right.”
That observation is often the starting point that gets someone tested, treated, and feeling better.
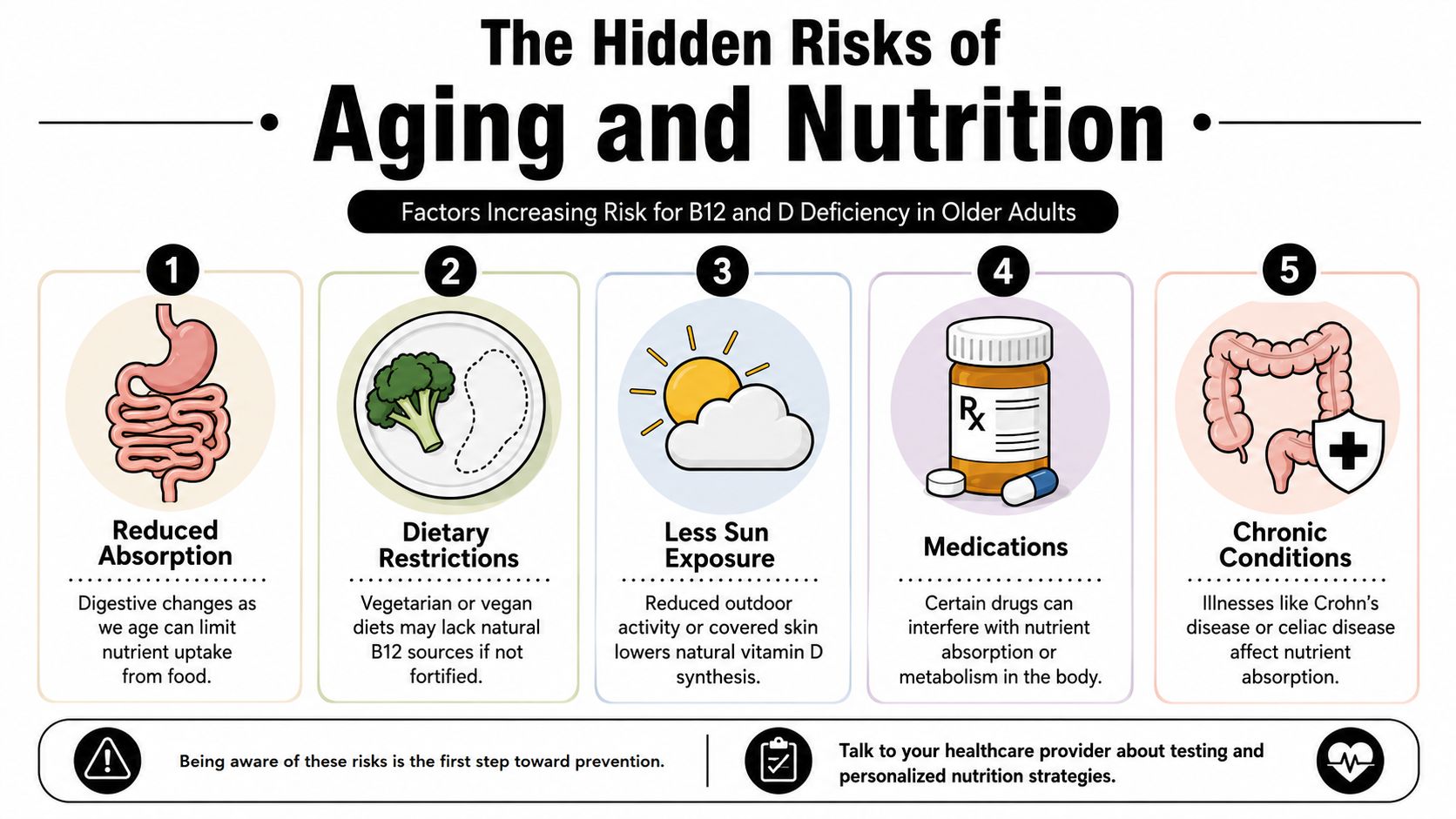
The Hidden Risks of Aging and Nutrition
Older adults don't become deficient because they “failed” at nutrition. More often, aging changes how the body gets and uses nutrients.
For vitamin B12, the issue often isn't just what someone eats. It's whether their body can absorb it. A clinical review in American Family Physician notes that vitamin B12 deficiency is widely recognized as a major global nutritional problem and affects about 20% of people over 60 in the US and UK. The same guidance says risk is higher in adults older than 75 and in people using metformin long term or taking proton pump inhibitors or H2 blockers for more than 12 months.
Why B12 becomes harder to absorb
Think of stomach acid like a key that helps release B12 from food. In many older adults, that key gets weaker. If someone also has long-term acid suppression, previous stomach surgery, digestive disease, or pernicious anemia, the body may struggle even more.
The practical point for families is this: someone can eat reasonably well and still end up low in B12.
Common situations that should make you more alert include:
- Long-term acid reducers: Omeprazole and similar medicines can make B12 absorption more difficult over time.
- Metformin use: Many older adults take it for diabetes and don't realize it can affect B12 status.
- Restricted diets: Vegetarian or vegan eating patterns may lower intake of natural B12 sources unless fortified foods are used consistently.
- Digestive conditions: Crohn's disease, celiac disease, or prior gastrointestinal surgery can interfere with absorption.
- Advanced age: The older the adult, the more cautious I'd be about assuming fatigue or memory changes are “just age.”
Why vitamin D drops so easily
Vitamin D risk looks a little different. It's tied to sunlight, time outdoors, skin production, diet, and overall health. A systematic review discussed in this open-access summary estimated that 14% of the global population had serum 25-hydroxyvitamin D levels below 30 nmol/L, which helped push vitamin D deficiency into routine public-health and primary-care discussions.
In day-to-day caregiving, the pattern is familiar. The older adult goes outside less, walks less, covers more skin, or lives in a setting with limited time outdoors. Add reduced dietary intake and chronic illness, and low vitamin D becomes easier to understand.
If bone health is already on your mind, this guide on optimising bone density for healthy ageing gives useful context for how nutrient status fits into the bigger picture of strength, falls, and fracture risk.
What caregivers can do this week
Don't try to diagnose from the kitchen table. Do start noticing patterns.
A simple caregiving checklist:
- Review medications: Write down every prescription, over-the-counter medicine, and antacid.
- Look at eating patterns: Is your relative eating less meat, fish, eggs, dairy, or fortified foods than they used to?
- Notice routine changes: Less walking, less sunlight, more sleeping in a chair, and fewer outings can all matter.
- Track function, not just symptoms: “Needs the railing now” or “stopped doing errands” is often more helpful than “seems weaker.”
- Support meals practically: If food variety is slipping, a routine like meal planning for seniors can help families spot gaps and reduce skipped meals.
Overlapping Symptoms and Common Lookalikes
Families often find themselves in a predicament. The symptoms overlap so much that it's hard to know what deserves testing.
Vitamin B12 deficiency can affect nerves, thinking, mood, and blood cells. Vitamin D deficiency is more often linked with muscle weakness, bone discomfort, and mobility problems, but fatigue and low mood can overlap. Aging itself can bring slower walking, less stamina, and occasional forgetfulness. Depression can flatten energy and motivation. Early dementia can affect memory and function. Arthritis can make someone move less and appear weak.
That's why symptom patterns matter more than any one complaint.
A major challenge for caregivers is that B12 deficiency can cause memory problems, low mood, and weakness before any signs of anemia appear, which can delay diagnosis and increase the risk of lasting nerve damage, as explained in the Merck Manual home guide on vitamin B12 deficiency.
Symptom checker
| Symptom Category | Potential Sign of B12 Deficiency | Potential Sign of D Deficiency | Often Mistaken For |
|---|---|---|---|
| Fatigue | Low energy, tiring easily | Low energy, reduced stamina | “Normal aging,” poor sleep, stress |
| Walking changes | Unsteady gait, balance trouble, odd foot sensation | Muscle weakness, slower rising, less confidence walking | Arthritis, deconditioning, fear of falling |
| Memory and focus | Brain fog, forgetfulness, slower thinking | Less common as a main clue, but low energy can affect focus | Early dementia, distraction, grief |
| Mood changes | Low mood, irritability, apathy | Low mood can overlap | Depression, loneliness |
| Numbness or tingling | More suggestive of B12 deficiency | Not a classic leading clue | Diabetes, spine issues, circulation worries |
| Aches and discomfort | Can happen, but not usually the main pattern | Bone or muscle discomfort, general achiness | Arthritis, inactivity |
| Weakness | General weakness, especially with nerve symptoms | Muscle weakness, trouble getting up or climbing steps | Frailty, “just slowing down” |
Clues that make me think harder about B12
I get more concerned about B12 when a caregiver reports a mix of:
- Tingling, numbness, or burning sensations
- Balance problems or new clumsiness
- Memory or personality change
- Fatigue that doesn't make sense
- A history of stomach issues, metformin, or acid-reducing medicine
That combination should move B12 higher on the list, even if no one has mentioned anemia.
Don't wait for pale skin or obvious anemia before asking about B12. Nerve and mood symptoms may show up first.
Clues that push vitamin D higher on the list
Vitamin D rises on my list when I hear:
- More trouble standing from a chair
- Generalized muscle weakness
- Aches that feel broad rather than joint-specific
- Reduced mobility and very little outdoor time
- Recent falls, near-falls, or new fear of walking
A practical example: if your aunt says, “My knees hurt,” that may be arthritis. If she also says, “My legs feel weak, I barely go outside, and I'm wobblier than usual,” vitamin D deficiency becomes worth discussing.
When symptoms are probably not just aging
Normal aging is usually gradual. Deficiency-related problems often get attention because the family notices a change.
Look for these patterns:
- The person has clearly declined over months, not years
- Multiple systems seem involved at once, such as mood, walking, and energy
- The explanation doesn't fully fit, such as memory changes plus tingling in the feet
- The person stops activities they used to manage, like shopping, bathing safely, or climbing stairs
If you're seeing that pattern, ask for evaluation. You don't need to prove the diagnosis first.
Navigating Blood Tests with Confidence
Your mother finally gets lab work after months of fatigue, weaker legs, and forgetfulness. Then the call comes back: “One vitamin is a little low.” For many families, that is where the confusion starts, not where it ends.
Lab testing helps separate “maybe this is aging” from “we need to treat this.” You do not need to become a clinician. You do need to know the test names, what a borderline result can mean, and how to ask one more question when the answer feels too vague.
The key B12 tests
For B12, the usual starting point is a serum vitamin B12 level. According to the Merck Manual professional reference on vitamin B12 deficiency, a clearly low serum B12 supports the diagnosis, and methylmalonic acid can help clarify the picture when the B12 level is borderline.
That middle zone causes trouble for caregivers. A result can come back “low-normal” or “borderline,” while the older adult still has numb feet, slowing, or new confusion. B12 works a bit like a fuel gauge that does not always match how the engine is running. If symptoms fit, a borderline number should lead to a closer look, not automatic reassurance.
Questions to ask at the visit:
- If the B12 result is borderline, should we check methylmalonic acid?
- Could poor absorption be part of the problem?
- Do any current medicines make B12 deficiency more likely?
- Do the symptoms suggest we should treat promptly while sorting out the cause?
The right vitamin D test
For vitamin D, the test name that matters is serum 25-hydroxyvitamin D [25(OH)D]. That is the form clinicians use to judge vitamin D stores.
Families often get tripped up here because “vitamin D was checked” sounds clear, but the exact test still matters. Writing down 25-hydroxyvitamin D helps you confirm that the right lab was ordered and makes follow-up conversations much easier.
If you like to review the basics before an appointment, this overview of a blood test for vitamin and mineral deficiency can help you get familiar with the wording you may hear in clinic.
How to keep results from slipping through the cracks
The blood draw is usually the easy part. The harder part is making sure the result leads to a clear plan.
I often see families run into the same problem. One person remembers, “The doctor said it was fine.” Another remembers, “They said to start something.” No one has the actual number, the test name, or the recheck date. That is how treatable deficiencies get mislabeled as just getting older.
Use a simple tracking system:
- Save the lab date
- Write the exact test name
- Record the result exactly as written
- Note what the clinician wants to do next
- Write down when the lab should be repeated
A shared folder, notebook, or printed sheet all work. If your family is keeping track of several appointments and specialists, this guide on how to organize medical records can make follow-up much easier.
Bring a symptom timeline to the lab review visit. “More forgetful lately” is easy to dismiss. “Became unsteady in November, foot tingling started in January, stopped driving in February” gives the clinician a much clearer picture.
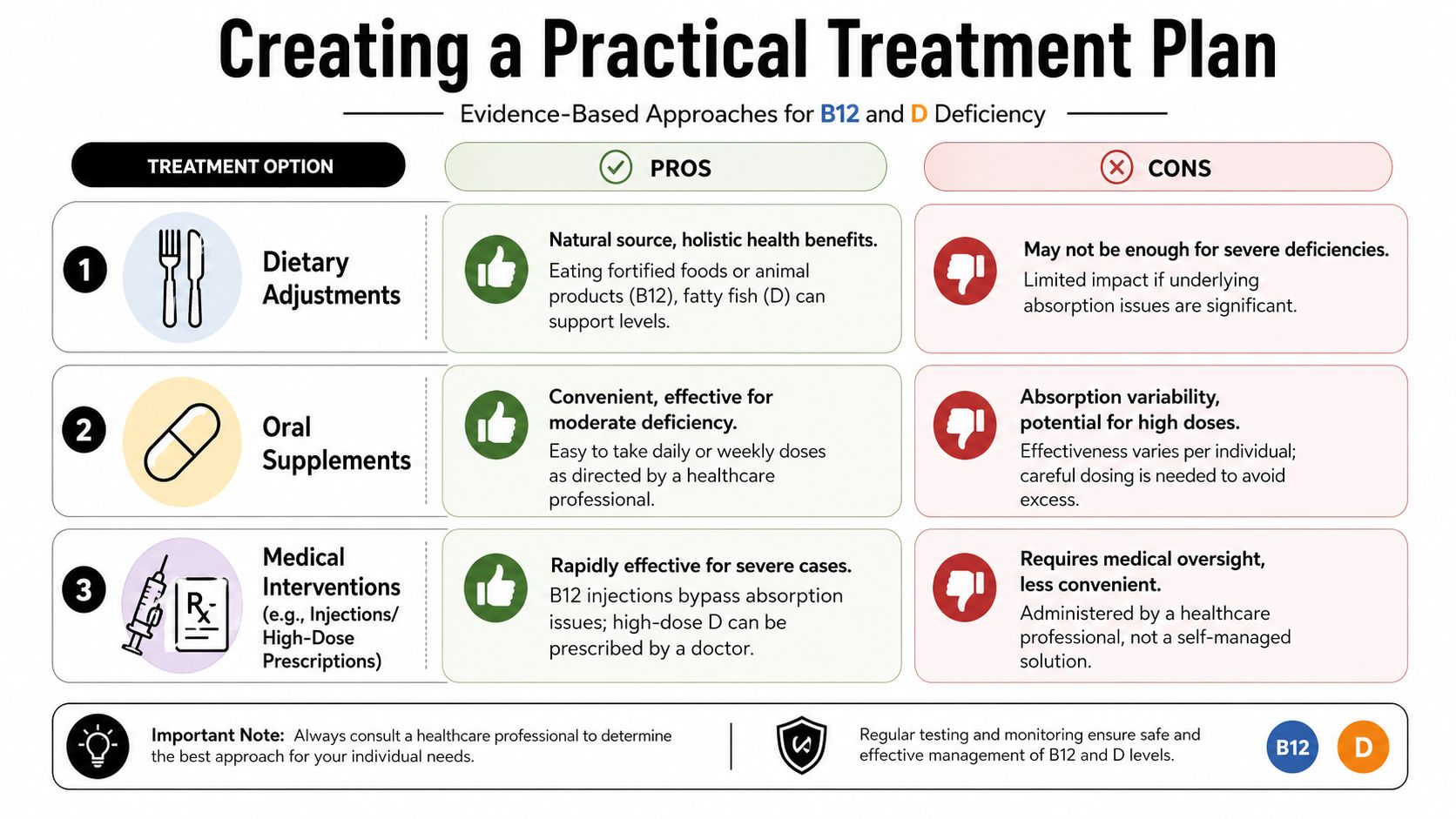
Creating a Practical Treatment Plan
A good treatment plan answers two questions at the same time. What deficiency are we treating, and why did it happen in the first place? That second question matters because a low lab value from poor intake is handled differently from a low lab value caused by poor absorption.
Caregivers often get stuck here. The symptoms may have looked like aging, depression, neuropathy, or “just slowing down,” and once the deficiency is found, families are relieved enough to assume any supplement will solve it. Treatment usually needs a little more structure than that.
Diet helps, but it has limits
Food is the foundation, especially if meals have become sparse, repetitive, or low in protein. B12 naturally comes from meat, fish, eggs, dairy, and fortified cereals. Vitamin D is found in fatty fish, fortified milk, and other fortified foods, though food alone usually does not supply enough vitamin D to correct a clear deficiency.
Diet works like refilling a pantry. It helps if the shelves are low. It does not solve the problem if the front door is jammed.
That is why an older adult can eat eggs, yogurt, or fish and still stay low in B12. Pernicious anemia, stomach surgery, intestinal disease, and some long-term medications can interfere with absorption. In that situation, advice to “eat better” is supportive, but it is not the whole plan.
Oral supplements and how they fit
Oral supplements are often the simplest starting point. For B12, clinicians may choose cyanocobalamin or methylcobalamin. For vitamin D, you will usually hear about D2 or D3.
Vitamin D treatment often has two phases. First, the clinician corrects the deficiency with a higher dose for a limited period. Then the plan shifts to a lower maintenance dose to keep levels steady. The exact dose depends on the lab result, kidney function, other medicines, fracture risk, and whether the person is likely to absorb and take it consistently.
Families should not copy a dosing schedule from the internet or combine several over-the-counter products without checking the total. That mistake is common, especially when a multivitamin, bone health supplement, and standalone vitamin D are all in the house. If your relative is also taking calcium, this guide to calcium supplements for older adults can help you sort out what belongs in the plan and what may be unnecessary duplication.
If you want a plain-language primer specifically focused on B12 for fighting anemia, that resource can help you understand why B12 gets discussed so often in fatigue and blood-count conversations.
When medical treatment is the better route
B12 injections are sometimes the better choice, especially when the body cannot absorb enough from pills or when nerve symptoms are already showing up. Families are often told “B12 is low,” then left to guess whether a store-bought tablet is enough. Ask the clinician to be specific about the route, the reason for it, and when improvement should be noticeable.
A clinician may favor injections or closer supervision when any of these are present:
- Pernicious anemia
- Clear malabsorption
- Significant neurologic symptoms
- Poor improvement on oral treatment
- Trouble managing a consistent daily regimen
The educational video below gives a useful overview of vitamin deficiency treatment concepts in plain language.
What a realistic plan looks like at home
The best plan is one a tired family can carry out on an ordinary Tuesday.
Keep it simple:
- One person maintains the current medication and supplement list
- Doses are tied to a daily routine, such as breakfast or the evening pillbox
- Symptoms are tracked in a few words, such as balance, appetite, tingling, mood, or stamina
- Everyone knows what improvement to watch for
- Everyone knows what should prompt a call back, such as worsening numbness, ongoing confusion, falls, or no clear progress
Improvement is not always dramatic. Some people feel less tired first. Others improve first in walking, steadiness, concentration, or appetite. If symptoms continue, do not assume the treatment “failed” or that the decline is only age. It may mean the dose, route, adherence, or even the diagnosis needs another look.
Long-Term Management and Safety
Once treatment starts, the work shifts from “What's wrong?” to “Is the plan working, and is everyone following the same plan?” That second part matters more than people expect.
Vitamin B12 problems can return if the root issue is ongoing. If the deficiency came from poor absorption, the person may need a long-term strategy rather than a short burst of treatment. Vitamin D also needs follow-through. Doses may change after the initial correction period, and rechecking helps confirm the person responded.
Safety matters more than enthusiasm
Families sometimes swing from underreacting to overreacting. They go from “it's probably nothing” to buying several bottles of supplements and doubling up.
That's not a good idea.
High-dose vitamin D should be guided by a clinician, especially when someone has kidney issues, multiple prescriptions, or a complicated medical history. B12 is generally handled differently, but the bigger issue is still accuracy. If symptoms continue despite treatment, the answer may be poor absorption, the wrong dose, poor adherence, or a different diagnosis altogether.
Keep the bottle, dose, start date, and prescriber in one place. That one habit prevents a lot of confusion.
Coordinating with the care team
The caregiver's job often becomes communication. One doctor orders testing. Another manages diabetes. Assisted living hands out pills. A home aide notices weakness. If no one shares the same update, treatment gets sloppy.
Use a short communication format:
- Diagnosis or concern: suspected or confirmed B12 deficiency, vitamin D deficiency, or both
- Current treatment: exact supplement or injection plan
- Monitoring: what symptoms the family is watching
- Follow-up date: when labs or visits are scheduled
- Red flags: falls, worsening confusion, poor intake, new numbness
If bone health support is also part of the plan, this guide on calcium supplements for elderly adults can help families think through how supplements fit together without turning the routine into guesswork.
What improvement can look like
Improvement isn't always dramatic. Sometimes it looks like:
- getting out of a chair with less effort
- fewer complaints of “pins and needles”
- better participation in meals or conversation
- fewer near-falls
- a return to familiar routines
What you don't want is silence and assumption. If the person seems unchanged, ask whether follow-up testing happened and whether the diagnosis still fits.
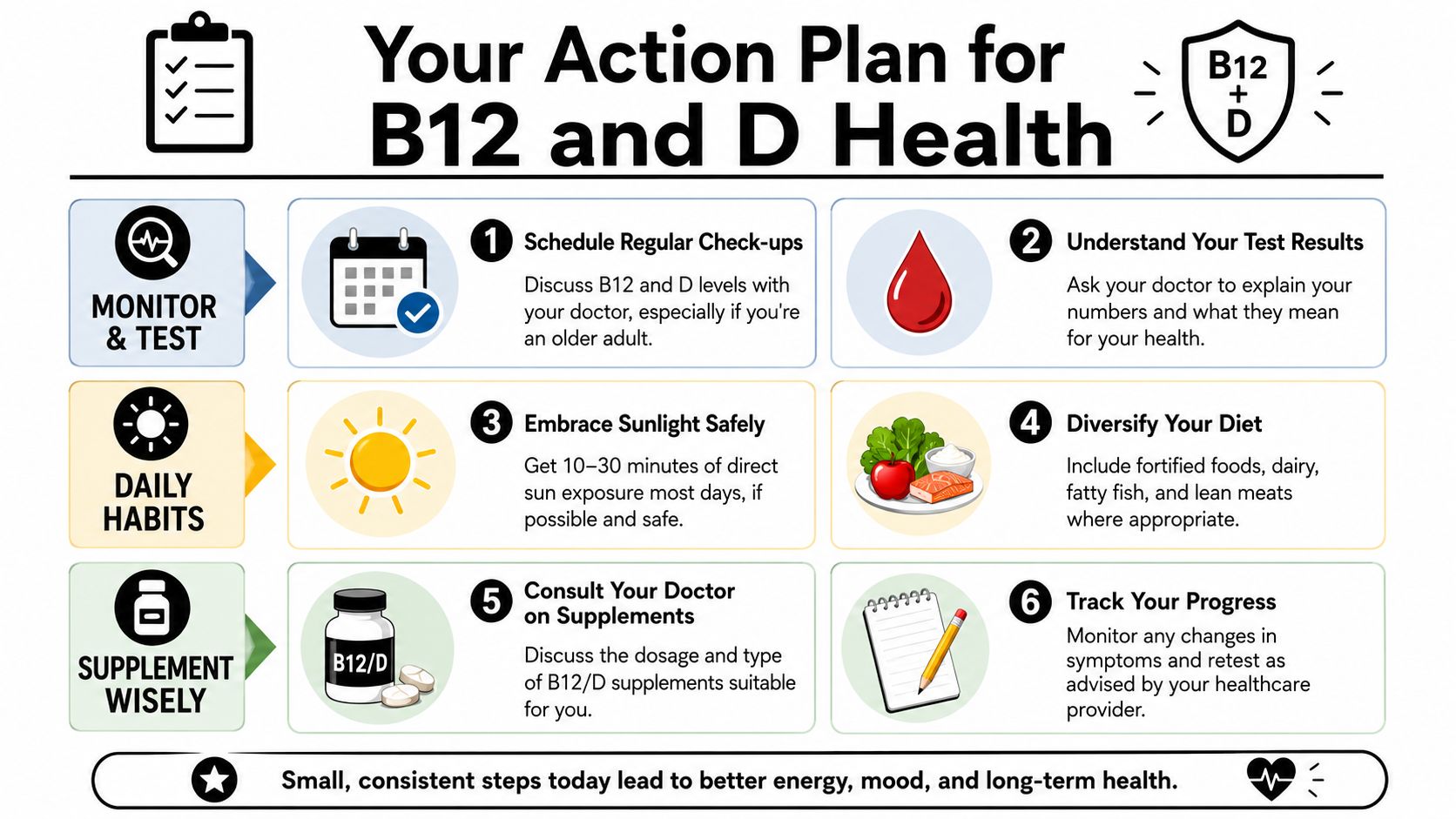
Your Action Plan for B12 and D Health
You don't need to solve this alone at home. You do need to trust what you're seeing.
If your relative has changed in a way that seems bigger than ordinary aging, bring that concern forward clearly. Caregivers are often the first people to spot the pattern. That pattern is valuable clinical information.
Red flags to discuss with a doctor
- New unsteadiness: especially if walking, turning, or stairs suddenly seem harder
- Persistent fatigue: not just one bad week, but an ongoing drop in stamina
- Memory slips with other physical symptoms: particularly when forgetfulness comes with weakness, tingling, or mood change
- Tingling or numbness: especially in feet or hands
- Low mood or withdrawal: when it feels new or out of proportion
- Very limited diet or long-term use of metformin or acid-reducing medicines
Next steps for caregivers
- Book the appointment. Don't wait for symptoms to become severe.
- Bring a medication list. Include prescriptions, antacids, vitamins, and supplements.
- Describe functional changes. Say “she stopped going outside” or “he needs help standing,” not only “she seems off.”
- Ask specific testing questions. For B12, ask whether a borderline result needs more evaluation. For vitamin D, ask whether serum 25-hydroxyvitamin D was checked.
- Write down the plan before leaving. Test names, treatments, and follow-up dates should be clear.
- Track what changes at home. Energy, walking, mood, numbness, appetite, and falls are all useful markers.
When families act early, they give their loved one a better chance at safer mobility, clearer thinking, and a better quality of life. That's not overreacting. That's good caregiving.
Family caregiving gets easier when you have practical tools, clear explanations, and a way to keep everyone on the same page. Family Caregiving Kit offers straightforward guides and decision tools designed to help you organize information, reduce overwhelm, and take the next step with confidence.